6.3 Impact of adults with mental illness on children they care for: Guidance
This procedure was updated on 26/02/24 and is currently uptodate.
Contents
- Executive Summary(Jump to)
- Context and aims(Jump to)
- Principles(Jump to)
- Consider the child/children's experience - what is life like for the child living with an adult with mental illness?(Jump to)
- Decision-making Flowchart(Jump to)
- Prompts for Considering Adults Capacity to Care for Children(Jump to)
- Guidance for referral to adult mental health services(Jump to)
- Guidance for referral to children's social care(Jump to)
- Joint working Between Agencies(Jump to)
- Joint Working & Risk Assessments(Jump to)
- Resolution of disputes and differences(Jump to)
- Addendum(Jump to)
- Possible effects of adult mental ill health on children(Jump to)
- Pregnant Women(Jump to)
- Substance Misuse, Mental Health & Domestic Abuse(Jump to)
- Related guidance and further information(Jump to)
- Related Policies, Procedures, and Guidance(Jump to)
Executive Summary
| 6.3.1 |
|
Context and aims
| 6.3.2 | This procedure has been written to improve the coordination and communication between all agencies in Buckinghamshire engaged with children and families and parents who have mental health needs. |
| 6.3.3 | The procedure should be applied whenever there are concerns about the well-being or safety of children whose parents or carers have mental health needs, specifically where these difficulties are impacting, or are likely to impact, on their ability to meet the needs of their children. This procedure also applies to pregnant women who have mental health problems or where their partners are known to have mental health problems. |
| 6.3.4 | The National Biennial Review of Serious Case Reviews (2014-2017) reported that 53% involved parents with mental health problems. In these cases the mental illness of the parent had a significant impact on their parenting capacity, resulting in the death or serious injury of the children. However, it remains the case that the majority of mentally ill parents do not harm their children. It also does not mean that parents who experience mental health problems have poor parenting skills. |
| 6.3.5 | However, the impact of parental mental health problems can, on some occasions, lead to children and families needing additional support; or, in a small number of cases, support and multi-agency action to prevent significant harm. |
Principles
| 6.3.6 | The guidance is underpinned by the following principles: All those who come into contact with children, their parents and families in their everyday work, including practitioners who do not have a specific role in relation to child protection, have a duty to safeguard and promote the welfare of the child as set out in Working Together to Safeguard Children.
|
Consider the child/children's experience - what is life like for the child living with an adult with mental illness?
| 6.3.7 | Here are some messages to mental health professionals written by young people from a Barnardo’s project in Liverpool2. The messages show how important it is to keep children informed. Introduce yourself. Tell us who you are and what your job is. Give us as much information as you can. Tell us what is wrong with our parents. Tell us what is going to happen next. Talk to us and listen to us. Remember it is not hard to speak to us; we are not aliens.
Tell us if there is anyone we can talk to. MAYBE IT COULD BE YOU. |
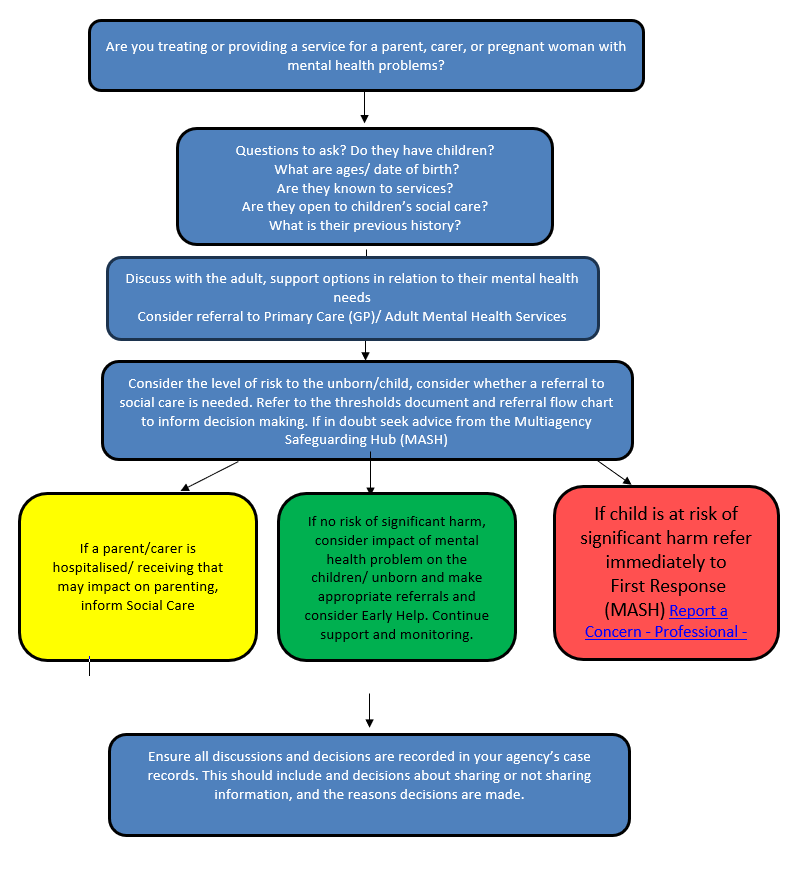
Decision-making Flowchart
| 6.3.8 | This flowchart is relevant to all services in Buckinghamshire which are treating or providing any kind of service to parents, carers, or pregnant women with mental health problems.
|
Prompts for Considering Adults Capacity to Care for Children
| 6.3.9 | Informed assessments and effective multi-agency/disciplinary working are the key to ensuring that children and families receive the appropriate services to meet their identified needs and manage risk. The key to ensuring children are safe, protected, and their needs are being met where parents/carers have additional needs, is to assess parent’s/carers capacity and ascertain if additional support is required. Consider the following areas:
Key questions Are parents/carers able to provide the following: BASIC CARE
ENSURING SAFETY
EMOTIONAL WARMTH
STIMULATION
GUIDANCE & BOUNDARIES
STABILITY
See Continuum Of Need for further information |
Guidance for referral to adult mental health services
| 6.3.10 | If there is concern about the mental health needs of a parent/carer, the adult’s Primary Cary Team/ GP should be contacted in the first instance and a request made for information to be shared regarding any existing or previous diagnosis of mental illness, and previous or current treatment or referrals. |
| 6.3.11 | In order for timely sharing of this information, the Primary Care Team will need to know why the information is needed, in what timescale it needs to be provided, with whom the information will be shared (within health professionals or with other agencies), what information is being asked and whether the patient has consented to this information being shared. |
| 6.3.12 | Practitioners should be aware that women in Buckinghamshire who are temporarily placed in refuges may be additionally vulnerable to their mental health needs not being met and patient information between systems may be limited. |
| 6.3.13 | If there is an imminent danger to the person or others, including a child, the police must be contacted. Staff must ensure that their decision and agreed course of action is fully and accurately documented. |
| 6.3.14 | Triggers that may indicate a referral to adult mental health services for initial assessment is needed are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
|
| 6.3.15 | Concerns should be discussed with the person’s Primary Care Team/GP in order to agree the most appropriate course of action. It would be usual practice for the Primary Care Team/GP to assess the client in the first instance and make a referral to mental health services if appropriate. However, in some circumstances another professional may make the referral, or the client may self-refer. |
| 6.3.16 | A past history of mental health problems will not necessarily mean a referral is required; this will depend on what the particular diagnosis was, current mental state, how long an individual has been stable and the level of support at home. |
Guidance for referral to children's social care
| 6.3.17 | In any instance where there is a concern about the welfare of a child, professionals should consult the BSCP Continuum of Need Incorporating Threshold Guidance. |
| 6.3.18 | A referral to Children's Social Care for an initial assessment or pre-birth assessment should always be made if a parent, carer or pregnant woman is considered to have significant mental health problems, as indicated by the triggers given below. A referral should always be discussed with a manager. |
| 6.3.19 | If there is an imminent danger to the person or others, including a child, the police must be contacted. |
| 6.3.20 | Speak to the family to discuss the concerns and reasons for referral. Gain a better understanding of the situation and gain consent to refer if possible |
| 6.3.21 | Think family – consider all family members including all the children. Risks may be relevant to some or all of the children in the family. |
| 6.3.22 | Consideration should be given to a referral to Early Help in order to provide additional support and safeguard children at an early stage. Early Help in Buckinghamshire is now provided by the Family Support Service. |
| 6.3.23 | Consider schools involvement – what support is school offering? Are they aware of the family situation? Is the school counsellor involved? Is the child’s school attendance level a concern? |
| 6.3.24 | Triggers that indicate referral to Children’s Social Care are listed below. However, this is not an exhaustive list and is provided to assist professional decision-making.
|
| 6.3.25 | Where a parent or carer expresses thoughts of self-harm, an assessment of risk to the child or unborn baby must be made and consideration given to a referral to Children’s Social Care based on the level of risk. Management of self-harm risk by adult mental health services staff must include in the plan actions to support the needs of the child/children/unborn baby and there should be discussion with the organisation’s lead for child safeguarding. Where necessary, advice should be sought from First Response. Consideration must always be given to the care arrangements for the children should the parent need to be admitted to hospital. |
| 6.3.26 | When a parent or carer has been receiving inpatient services, in whatever setting, consideration must be given to discharge arrangements to ensure provision for the children is appropriate, and their welfare and safety has been properly assessed. A formal meeting with Children’s Social Care should be held where they are already involved or if concerns are identified. If a parent or carer discharges themselves out of hours, a referral to the Emergency Duty Team should be made to ensure the children's welfare is protected. |
| 6.3.27 | Newly identified risk or changes in the risk assessment in any agency must be communicated to other relevant agencies in order that they can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of the family might have impact on another member, and that a Think Family approach is essential. |
| 6.3.28 | Where the need for referral to Children’s Social Care is unclear, this must be discussed with a line manager and/or safeguarding lead. Children’s Social Care can be consulted for advice. Staff must ensure that all decisions and the agreed course of action are signed and dated, and that a written referral using the MARF (multi-agency referral form) follows any telephone conversation or referral. If a referral is not made, the reasons must also be clearly documented. |
Joint working Between Agencies
| 6.3.29 | All information should be shared in line with the BSCP Information Sharing Code of Practice and HM Government advice. |
| 6.3.30 | It is essential that staff working in adult mental health and children’s services work together to ensure the safety of the child and the management of the adult’s mental health. |
| 6.3.31 | Joint work will include mental health workers providing all information with regards to:
|
| 6.3.32 | Parents/Carers with mental health issues entrust professionals with, or allow them to gather, sensitive information relating to their health and other matters as part of their seeking treatment. They do so in confidence and they have legitimate expectation that staff will respect their privacy and act appropriately. |
| 6.3.33 | Where there are concerns about the wellbeing of a child, the need to share information will take precedence over the patient’s right to confidentiality. However, practitioners need to consider what information is and is not confidential, and the need in some circumstances to make a judgement about whether confidential information can be shared, in the public interest, without consent. |
| 6.3.34 | Sensitive information can be shared if there is a clear and justifiable purpose, and consideration has been made of the safety and wellbeing of the child and others who may be affected. The more sensitive the information, the greater the child focus needs to be in order to justify sharing. |
| 6.3.35 | The practitioner needs to be mindful that information may need to be shared with a number of agencies, therefore the ‘need to know’ and ‘proportionality to the risk of harm’ principles apply. Where a practitioner is considering the inclusion or exclusion of sensitive information, or consent has been refused, they must discuss this with their safeguarding lead within their organisation. If an adult’s clinical information is shared without their consent, the adult should be notified of this.
For further guidance please see: Information Sharing - Buckinghamshire Safeguarding Children Partnership (buckssafeguarding.org.uk) |
| 6.3.36 | Child protection workers must assess the individual needs of each child and, within this, incorporate information provided by mental health workers. They must assess the risk and impact on each child in accordance with information provided by mental health workers and the assessment framework. |
| 6.3.37 | Mental health professionals must attend and provide information to any meeting regarding the potential impact of parent/Carer mental health concerns on the child. These will include:
|
| 6.3.38 | Relevant professionals from Children’s Services and other agencies supporting the child should attend Care Programme Approach (CPA) and other meetings related to the management of the parent/carer’s mental health where concerns about capacity to parent have been raised. |
| 6.3.39 | All plans for a child, including Child Protection Plans, will identify the roles and responsibilities of mental health and other professionals. The plan will also identify the process of communication and liaison between professionals. All professionals should work in accordance with their own agency procedures/guidelines and seek advice and guidance from line management when necessary. |
| 6.3.40 | Key examples of good practice in joint working:
Consideration to be given to the adult’s accommodation history, have they always lived in Buckinghamshire, have the child/children been known in another local authority? |
Joint Working & Risk Assessments
| 6.3.41 | It is important to be aware that risk assessment in mental health work and risk assessment in child protection work are two different concepts, and it can be dangerous to confuse them. |
| 6.3.42 | The former is concerned with predicting the likelihood of a patient’s mental health deteriorating to the point where she/he poses a risk to self and/or others. The latter involves the analysis of information to consider whether or not the children’s likely experiences are acceptable, in terms of risk of physical or sexual assault, omission of care or neglect, or threat to emotional wellbeing. |
| 6.3.43 | Newly identified or changes in risk in one agency’s assessment must be communicated to other relevant agencies, so that they too can consider if this new information impacts on their own risk assessments. Staff must always consider that a change for one member of a family might have impact on the other member – a ‘think family’ approach is essential. |
Resolution of disputes and differences
| 6.3.44 | In the event of a dispute or disagreement arising between professionals, the BSCP Procedure for Escalation, Challenge and Conflict Resolution should be followed. |
| 6.3.45 | Any disagreements or differences should be recorded on the case file, including the views of the other party. |
Addendum
Possible effects of adult mental ill health on children
| 6.3.46 | Mental ill health can sometimes lead to neglect of both the adults and their children’s physical, emotional and social needs. The children may have caring responsibilities, which are inappropriate to their age and may have an adverse impact on their development. Some forms of mental ill health may cause adults to be ‘unavailable’ or not responsive to the child; or to behave in bizarre, unpredictable or violent ways towards themselves, their children or environment |
| 6.3.47 | The stigma and oppression associated with adult mental ill health can impair the adult’s ability to care for the child/ren and children can carry the burden of covering for parental behaviour. It can be difficult for adults to share their situation and struggles. Children may be reluctant to talk about family problems or seek support. Practitioners need to be sensitive to this. Refer to the ‘Child’s Experience’ section |
| 6.3.48 | At the extreme, a child may be at risk of severe injury, profound neglect or even death. |
| 6.3.49 | An adult carer’s mental ill health will be less likely to have an adverse effect on a child when:
|
| 6.3.50 | A significant history of violence is a risk indicator for children, as is parental non- compliance with services and treatment. |
| 6.3.51 | Children most at risk of significant harm are those who:
|
| 6.3.52 | The following factors may impact the ability of an adult to provide appropriate care and increase concerns that a child may have suffered, or is at risk of suffering, significant harm:
|
Pregnant Women
| 6.3.53 | When an agency identifies a pregnant woman experiencing mental health problems, an assessment must be undertaken to determine what services she requires and the BSCP Pre-Birth Procedures must be followed. |
| 6.3.54 | This must include gathering relevant information from their Primary Care Team/GP, in addition to any other agencies involvement, to ensure that the full background is obtained about any existing or previous diagnosis, or treatment for mental illness or substance misuse. This is especially important where service awareness of earlier births may need to be clarified, for example, in the case of older or overseas children. If a person has moved recently, it is advisable to seek out health records from the previous Primary Care Team/GP. It is also important to identify partners of pregnant women who have mental health or substance misuse problems. |
| 6.3.55 | Pregnant women in Buckinghamshire now book their maternity appointments online and these are coordinated by midwives based at the hospital and not by Primary Care Teams/GPs. As such, it is possible that a pregnant woman may not see her GP during the pregnancy and the first contact with their GP may be at the face-to-face six-week post-natal appointment. It is important that those working with pregnant women do not assume that the pregnant women are being routinely seen by their GP. |
| 6.3.56 | Research has shown that pregnant women with a previous history of mental health needs are particularly vulnerable to breakdown during the later stages of pregnancy and following the birth of their baby. |
Substance Misuse, Mental Health & Domestic Abuse
| 6.3.57 | When a parent has a substance misuse problem, as well as mental health needs, this can put the child at particular risk, especially where the potential for dealing with the substance misuse problem is limited. Where a parent/carer has mental health and substance misuse issues, the assessment of the parent should ideally be conducted in partnership between the Mental Health Care Management Team and the Adult Substance Misuse Care Management Team. |
| 6.3.58 | In addition, both the triennial review (2014--17) and previous biennial reviews of Serious Case Reviews have shown that the three issues of domestic abuse, parental mental ill health, and alcohol or substance misuse are not the only risk factors that may contribute to cumulative risk of harm. Other risk factors often co-exist with these factors, and potentially interact with them to create harmful environments for the children. These include issues such as adverse experiences in the parent/carer’ own childhoods, a history of criminality - particularly violent crime, a pattern of multiple consecutive partners, and acrimonious separation. Professionals should be aware of this when undertaking an assessment of risk. |
Related guidance and further information
- NSPCC, Parenting with a mental health problem
- Ofsted (2013) What about the children?
- Royal College of Psychiatrists (2011) Parents as Patients: supporting the needs of patients and their children
- Dept of Education: Learning for the future: final analysis of serious case reviews, 2017 to 2019 December 2022
- Oxford Health NHS Foundation Trust provide services such as psychological services, Adult Mental Health Teams (AMHT), complex needs service, Bucks Community Eating Disorders Team (BCEDT) and adult mental health inpatient services.